Oct 2022 updates: “antigenic” sharpened to Animal Challenge Immunofluorescence Testing (ACIT).
I can’t put into words how much I appreciate the opportunity my customers and colleagues afford me to expand upon and collaborate to advance the information state of the art in [1] which emerged in part via an informal notion at an older post [2]. Perhaps growing numbers of epidemiological researchers and related practitioners will digest this new information and pay more comprehensive attention to the actual seasons, along with quantitative metrics thereof. This, and hopefully slavish attention to ensuring that all geospatial and other considered populations are mutually exclusive unless otherwise noted.
SEASONAL POLLEN, INFLUENZA LIKE ILLNESSES (ILI), AND MUTUALLY EXCLUSIVE POPULATIONS (MEPS)
Reference [1] includes an exploration of the mechanisms by which viruses circulate within our hydrogeostrophic atmosphere, according to seasonal forcing. The paper relates this to vaccine program efficacies and to other candidate immunogens as pollens. All of that featured work relied in great part on some confidence that the data were possible to subdivide into mutually exclusive populations.
Here’s an except from Figure S6 of [1] regarding some of the diverse pollen categories that were examined at top and the geospatial distribution within New Mexico of the once ecumenical Influenza Like Illness (ILI) categories at bottom:
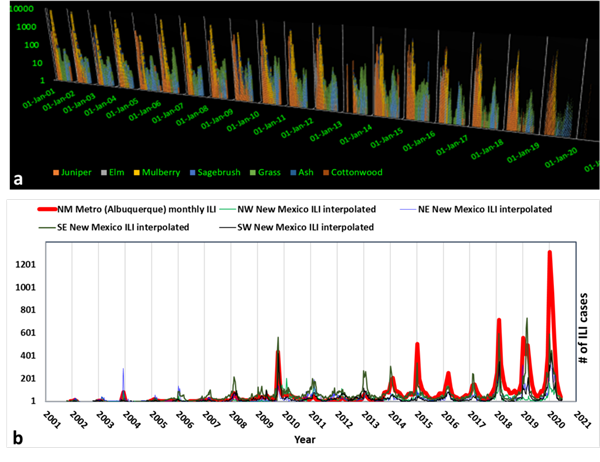
The two charts can be seen in full resolution in the Supplementary Material which can be downloaded at [1]. Again, both of these charts, along with the entire paper, assume intrinsically high confidence that various populations are mutually exclusive. In the examples above, the pollen species are easily separated into mutually exclusive host categories. In the bottom frame, the State of New Mexico is subdivided into 5 mutually exclusive geographical zones.
The paper wouldn’t be reliable if double-counting of ILIs were somehow extensive. You can’t count the influenza cases in Southeast New Mexico while you are tabulating the NM Metro (Albuquerque) cases. Mutually exclusive populations (MEPs) are critical in every possible direction a scientist can imagine. Unfortunately, because ILI surveillance (the Right Size Roadmap, RSR, which typically included coronaviruses) was curtailed this flu season, there is no longer any confidence that the populations of ILI are mutually exclusive from Covid-19 reports.
RESPIRATORY VIRUS MEPS may be IMPOSSIBLE TO DEFINE WITHOUT Animal Challenge Immunofluorescence Tests (ACITs)
I have used the ACITs term synonymously with the “antigen” term. This is not a convention adopted by PCR advocates but at times both PCR and ACITS appear to have been unreported. The NSR paper [1] also may recognize indirectly that Covid-19 is not routinely measured through “antigenic” testing. That study suggests that antigenic testing would be the best way to begin to return to the RSR protocols. Those protocols would be critical for any to confirm that populations of reports of actual Covid-19 illness are based on MEPs of respiratory viruses.
All might find it useful to know that under the previous RSR protocols, the healthy were not apparently tested under pandemic or normal seasons. The healthy were not tested, and statistically helpful proportions of the ill were antigenically tested for more than one viral strain. None of that appears to have survived as of early Spring of 2020, anywhere around the world (as other countries under the WHO followed a similar RSR protocol path).
The new MEP – defying viral alerts also seem dependent on a metaphor that relatively speaking, influenza viruses are docile canines, while Covid-19 breeds are somehow far more aggressive. Except they refer to these various viruses as different species and not breeds. I’ve taken some mild interest, purely as a nanoscientist, in the representations that these ILIs somehow asexually procreate, just because they need a host to thrive in. There may be some more to learn regarding this because the viral mutationists only seem to use the same cladistics and phenology tools that dog breeders use.
The highly sensitive PCR and related genetic testing were not originally contemplated to replace antigenic profiling. And those PCR approaches will never work while only healthy people are tested, and only for one virus breed. How do the hospital numbers signify Covid-19 patients? Unless they are conducting and reporting antigenic tests for all respiratory virus candidates, there may be no justification to signify with any weight that the numbers being reported to all are MEPs.
It may be that physician opinions are now permitted to tip the scales against antigenic testing protocols. Health care professionals might be more routinely afforded this subjective prerogative, now that the RSR has been curtailed. Perhaps some clinicians and their hospitals believe that any number of PCR tests are substitutes for the suite of antigenic tests, even if that doesn’t assure MEP conditions. They should submit their own paper to a good peer review journal to support, and cite this post or [1] as the impetus. Otherwise, without the broad statistically – informed support of an RSR-aligned data resource, it appears to remain impossible to attribute a viral strain as the cause of any respiratory illness without support from broad spectrum antigenic testing including ACIT, Animal Challenge Immunofluorescence Testing.
PEER REVIEW PAPERS ARE LACKING TO SUPPORT ACIT-FREE, MEP-CHALLENGED COVID-19 VACCINES AND DIAGNOSES
All clinicians and other health professionals should wait for peer acceptance of their antigen-free testing notions before they bean count another Covid-19 morbidity, case or mortality, or immunogenic success story, without including scientifically-based ACIT testing. The peer review process could take anywhere from one day to a decade in our world. But they should wait. The MEP question for antigenic strain equivalents relates also to the healthy. It’s a departure from the RSR to test only the healthy. But if the healthy are to be tested routinely, why is this population tested for only one strain? Why aren’t broad spectrum ACIT tests applied?
This also raised a question to me of whether or not full suites of ACIT tests are used and reported in all vaccine efficacy studies. Papers such as [3] offer a helpful starting point to compare how current vaccine claims and studies measure up. It is relevant because it considered the previous swine flu pandemic of 2009 to 2010. In that paper, the entire exercise of estimating vaccine efficacy (VE) was grounded in antigenic testing. That is summarized: (my bold and color): “During the study period, we detected 334 cases of influenza A H3N2, 373 cases of influenza A H1N1, and 333 cases of influenza B. All viral isolates assessed at the CDC for antigenic relatedness to the vaccine strains by hemagglutination inhibition tests using postinfection FERRET antisera were antigenically similar to the vaccine strains.”
Meanwhile, those who manage our avalanche of subsidized Covid-19 vaccines, along with the mandates, appear to have insufficient interest in both the RSR and ACIT testing. A recent paper focuses on the Pfizer vaccine [4] and appears to claim that this vaccine is very effective. Yet, I could not identify any mention of antigens in their study. Nor could I locate a rationale of why antigens and/or ACITS are not needed. It makes little sense, given that prior respiratory VE test-negative studies apparently always relied on such testing. If it is impossible to attribute a viral strain as the cause of a respiratory illness without ACIT testing, then why do all accept the VE claims? A peer reviewed publication that explains why antigenic testing is no longer necessary, might add value.
CASE STUDY: 500,000 INFLUENZA CASES REDEFINED AS COVID-19 CASES BY CDC.
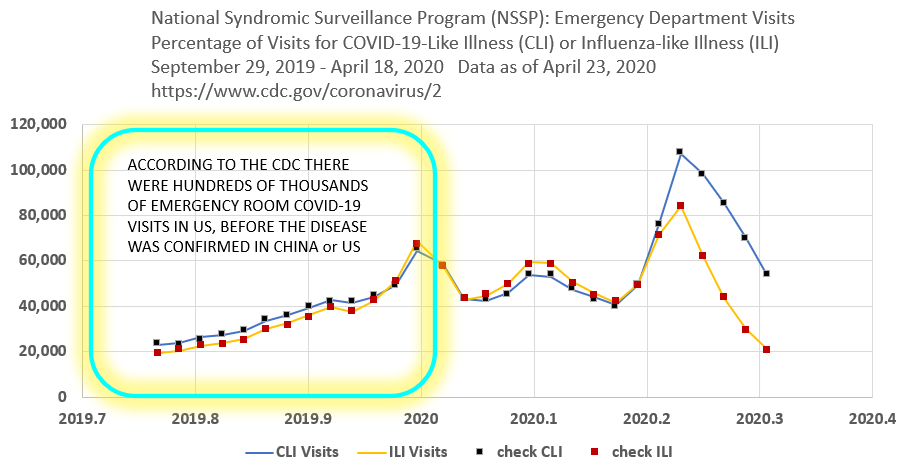
In this example below, a significant proportion of ILI numbers have been redefined by the CDC as Covid-19 Infected numbers. This has never been publicized or explained.
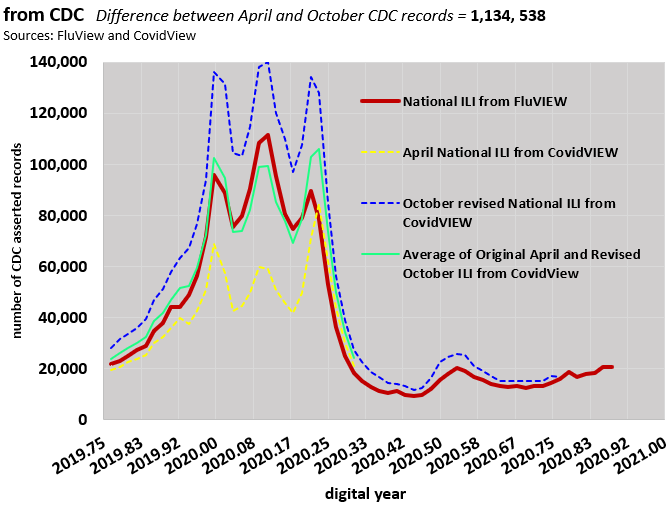
The images above and below also show that Covid-19 is attributed by the CDC to have reached the US by September 2019. That doesn’t match mainstream numbers and remains unexplored territory for epidemiologists.
HIGH FLYING SEASONAL VIRUSES AND MEPS
The success of [1], at least in reaching a publication goalpost, depended in great part on reproducible and mutually exclusive data definitions. This applied also to the geostrophic climate elements of the study, including its discussion of a seasonal sedimentation of once high-circling viruses to the surface every July and August in the darker shades of the Northern Hemisphere (lower geostrophic wind magnitudes) in this supporting graphic:
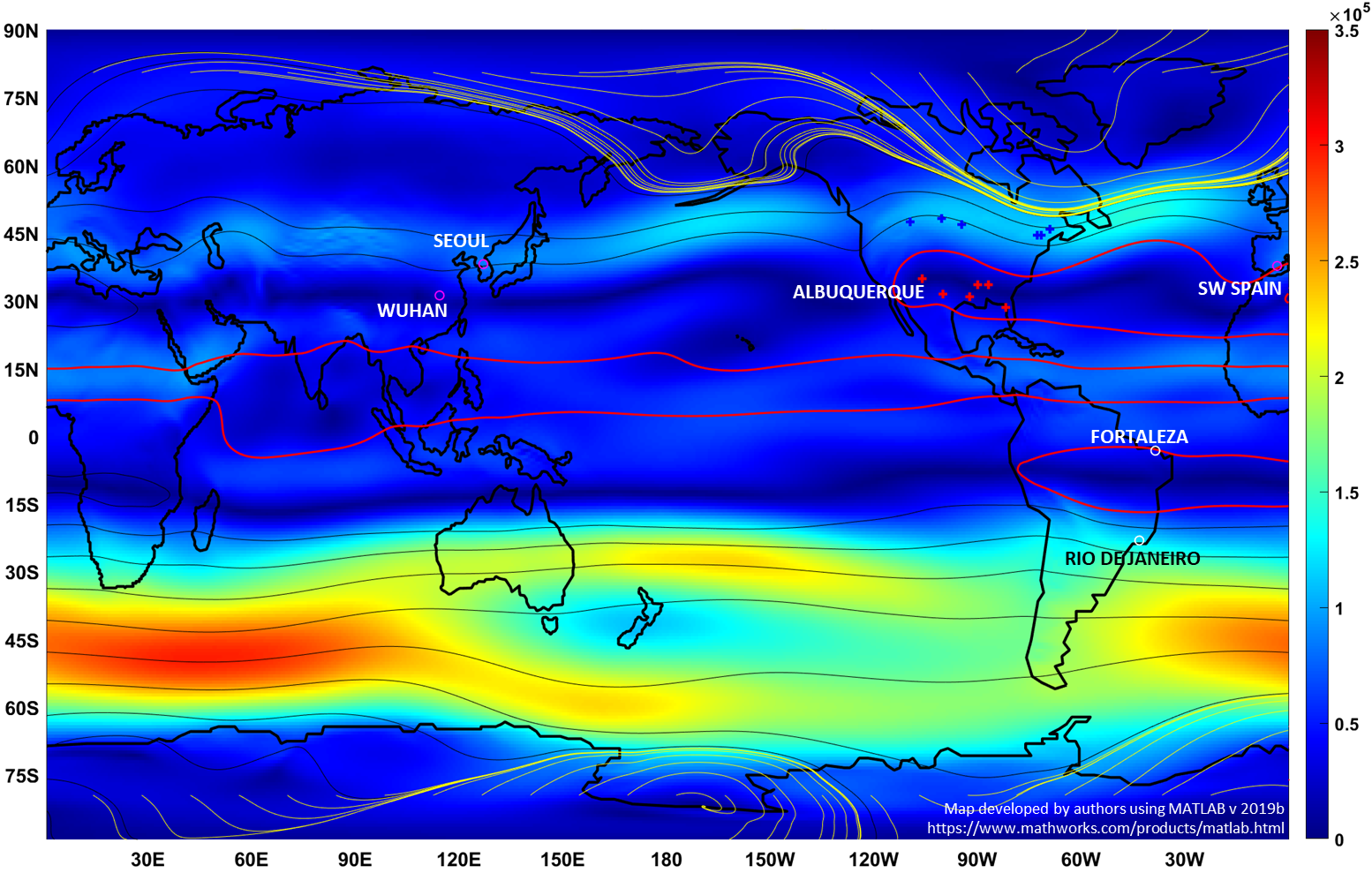
These plots were developed for a signature month of each season and those are also available at the link to [1]. One will then be able to begin to confirm in the context of the study that late summer Northern Hemisphere geostrophic winds are a MEP compared to the other featured seasons. The paper relates that late summer in the northern hemisphere is a significant period of virus and other aerosol sedimentation. This is a relatively unexplored concept, but all are welcome to visit that report and contemplate the additional pollen connections.
Finally for now, the image below is directly from a section of [1] and notes populations of seasonal respiratory coronaviruses whose strain identities were informed by antigenic testing. As noted in [1], the 2020-2021 flu season will not include RSR certified mutually exclusive respiratory viral populaton (MEP) information, and that this poses a data information obstacle to future studies in this direction.
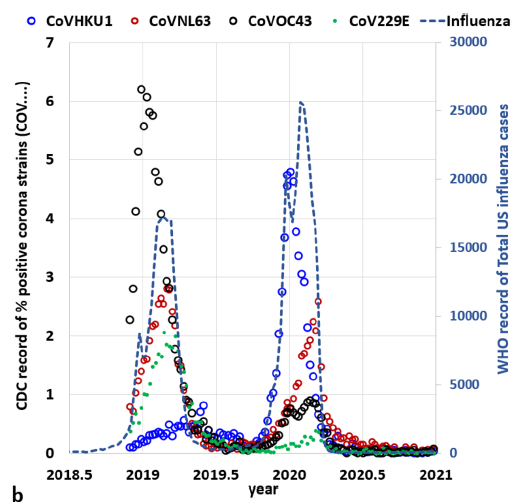
4 separate coronavirus strains (Source: CDC42)
and all influenza strains (Source WHO43). after [1]
THE ANTIGENIC DRIFTERS
The term “antigenic drift” is widely applied to Covid-19’s follow up strains such as the Delta Variant. This is a contradiction in terms, because none of those appear to have been verified through antigenic and/or ACIT tests.
A POSSIBLE WAY BACK TO THE RIGHT SIZE ROADMAP (RSR) or a commodity equivalent
Consider exploring this topic with others, including friendly neighborhood health care providers and lawmakers. ACIT tests are indispensable. And no matter what strains of ILI or CLI emerge from this point forward, ACIT tests can easily be developed for those as well. The RSR seeks a merger of best tests with parsimony and transparency. The current departure from the RSR seems unsustainable and unacceptable. Perhaps comprehensive ACIT test kits will become widely distributed over-the-counter. Along with the immediate restoration of the RSR, those might go a long way to bring us back to some balance,
REFERENCES AND CITATIONS
Featured Image fair use adapted from numerous representations of viruses and one representation of dogs by Artist Arthur Sarnoff (d. 2000). See https://en.wikipedia.org/wiki/Arthur_Sarnoff
[1] Wallace, M.G., and Wang, Y. 2021 Pollen antigens and atmospheric circulation driven seasonal respiratory viral outbreak and its implication to the Covid-19 pandemic. Nature Scientific Reports published August, 2021
[2] Wallace, Michael 2020 Climate, Influenza, Buffalo Bill, and a notion about pollen Abeqas post March, 2020
[3] Treanor, J.J. et al. 2012 Effectiveness of Seasonal Influenza Vaccines in the United States During a Season With Circulation of All Three Vaccine Strains Clinical Infectious Diseases 2012 55 (7) pp. 951-959
[4] Bernal, J.L. et al. 2021 Effectiveness of the Pfizer-BioNTech and Oxford-AstraZeneca vaccines on covid-19 related symptoms, hospital admissions, and mortality in older adults in England: test negative case-control study. BMJ 2021; 373 doi: https://doi.org/10.1136/bmj.n1088 (Published 13 May 2021)
This is a blog post that includes opinions